HUMAN MICROBIOLOGY
FUNGI AS PARASITES:
The impact of fungi on humans is potentially considerable when one considers the possible targets. As
parasites fungi primarily infect plants, and the Irish famine of the 1850s in which the potato crop was
ruined by Phytopthera infestans represents an alarming example of the damaging effects fungal infection
has on foodstuffs. Two million people died during the five-year period in which the crops were lost.
Less dramatically, fungi also cause spoilage of pharmaceutical and cosmetic products, as well as
attacking the timbers of our homes.
Only a small proportion of fungi (<0.1 per cent) exist as parasites of humans and animals, fungi mostly
acting as saprophytes (organisms that absorb their organic nutrients from dead substrates). By definition,
then, saprophytic organisms are not parasitic because their nutritional sources are not alive; instead the
organisms are acting as decomposers and recyclers. As most fungal infections are acquired from an
environmental source, fungi are not obligate human parasites but, instead, human mycoses can be
considered accidental infections that are not designed to facilitate the spread of the organism to new
hosts. Hence, human to human spread is very rare for most fungal infections with the exception of the
dermatophytes.
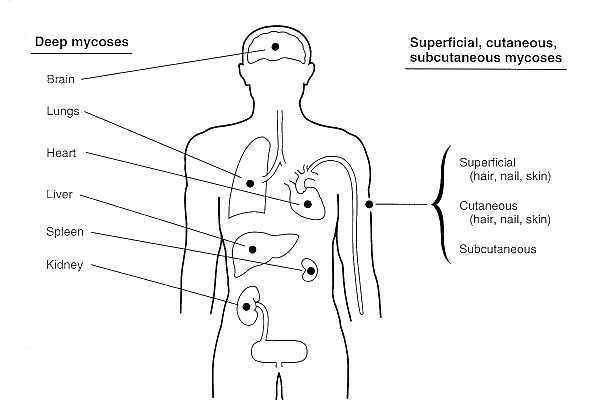
Clinically, human fungal infections can be grouped into:
(i) systemic disease(infections of internal organs of the body), and
(ii) localised or superficial infections (infections confined to the skin or mucous membranes that do not invade into deeper tissues or organs. This classification is anthropomorphic
in that it considers the diseases as they affect man. In order to see what are the important features
of the fungi themselves, it is appropriate to group the organisms into diseases by primary
pathogenic fungi and secondary pathogenic fungi. The tiny fraction of fungi that can cause
human disease, despite the daily exposure to large numbers of airborne fungal spores, can be
taken to mean that most fungi cannot overcome human defence mechanisms.
PRIMARY PATHOGENIC FUNGI:
The fungi that are primary pathogens are those that can infect and cause disease in healthy people;
‘healthy’ in that there are no recognisable predisposing features which facilitate infection. The diseases that are seen may be systemic infections or superficial infections. This immediately demonstrates how the severity of the infection is not necessarily an indication of the pathogenic potential of the organism.
Mycosis Aetiological agent(s)
Systemic mycoses
Histoplasmosis Histoplasma capsulatum
Systemic candidosis Candida albicans
Cryptococcosis Cryptococcus neoformans
Aspergillosis Aspergillus spp.
Localised infections
Dermatophytoses Epidermophyton spp., Trichosporum spp., Microsporum spp.
Candidiasis Candida albicans
Pityriasis versicolor Pityrosporum spp
SYSTEMIC INFECTIONS:
Fungi that are able to cause systemic illness in healthy people are rare and confined to specific
geographic locations across the world. The fungus Histoplasma capsulatum causes histoplasmosis
which is endemic to certain areas in the southern states of America. Another infection is
coccidiomycosis, caused by Coccidioides immitis. Like histoplasmosis, the fungus is found between the
southern states of America, Mexico and the northern-most countries of South America. These two
infections are caused by inhalation of the fungus, which exhibits dimorphism, i.e. can exist as a yeast or
a mould. The organisms are acquired by inhalation of the conidia from soil, and develop in the lungs as
yeasts. The ability to switch between forms is seen following the change in temperature so that
Histoplasma capsulatum is a mould when grown at 25°C but grows as yeast at body temperature. This
property is then more accurately described as thermal dimorphism. The switch from being a mould in
the soil where it adopts a saprophytic existence to a yeast when at 37°C presumably favours the parasitic
existence in a warm-blooded animal. Dimorphism is a particular feature of the endemic fungi that cause
systemic infections but it is not restricted to pathogenic fungi.
SUPERFICIAL INFECTIONS: THE DERMATOPHYTOSES:
The infections caused by the group of fungi collectively termed the dermatophytesare best known by
the infection ringworm. Nothing to do with worms, ringworm is a fungal infection of the skin which
shows up as a circular area of redness in which the fungal mycelia are radially extending outwards
through the superficial skin squames. The sites of infection are reflected in the medical terms tinea
barbae (beard), tinea capitis (head), tinea corporis (body), tinea cruris (groin), tinea pedis (foot) and tinea
unguinum (nail). The different sites of infection on the body reflect the ability of dermatophytes to
invade keratinised tissues (skin, hair and nails) but no further, since these fungi have the ability to obtain
nitrogen from the keratin present only in the (dead) tissues in the body.
The dermatophytes are a group of approximately 40 species that are classified by their anamorphic
(asexual) stages. They fall into three genera: Trichophyton, Microsporum and Epidermophyton within
the Fungi Imperfecta (Deuteromycota). The ability to reproduce sexually is very rarely found in these
organisms, and this is thought to represent the intermediate transfer from environmental organisms to a
strictly parasitic existence on humans and animals. The organisms can be described according to their
ecological location:
• anthropophilic dermatophytes: exclusively infect humans,
• zoophilic dermatophytes: animal parasites that accidentally infect humans,
• geophilic dermatophytes: soil inhabitants that can infect humans and animals.
As zoophilic dermatophyte infections are transmissible from animals to humans, anthropophilic
infections are transmissible from person to person, a property unusual in human mycoses. In addition, the organisms vary in their geographical distribution with some widespread (globally) and others restricted to specific areas of the world.
As the dermatophytes infect only keratinised tissues, they do not invade living tissues. In keeping with
the descriptions of radial growth, the lesions radiate as a ring with the advancing hyphae
migrating into new tissues, and the pathology shows varying degrees of cell-mediated inflammation with
an increased rate of division and keratinisation of the skin layers. This increased cell turnover will
provide an increased supply of nutrients for the fungus. The infections with the most degree of
inflammation are the zoophilic and geophilic species, unlike the anthopophilic infections, which are
often asymptomatic. Such findings support the idea that the most host-adapted species (the
anthropophilic species) are better suited to maintaining itself within a human population.
SECONDARY FUNGAL PATHOGENS:
The three fungi that we will consider are all able to cause systemic infections, but it appears that
predisposing factors in the host are required for secondary pathogenic fungi.
It is because of the advances in medicine that opportunistic infections have become a greater problem,
both in incidence and clinical management of the patient. The increase in the number of successful
organ transplants, for example, means that such patients are at risk of developing infections due to
opportunist organisms, of which fungi have been particularly problematic. We will consider three fungi
that have become regular culprits in causing infections in patients with underlying disease: Cryptococcus
neoformans, Aspergillus spp.and Candida albicans. In all three organisms, the increased opportunities
for invading the patient have arisen from the following factors:
• increased numbers of patients with immunosuppression: naturally occurring such as AIDS or
through more successful medical immune manipulation during transplantation.
• continued use of broad spectrum antibiotics.
• increased use of intravenous lines.
• increased rates of survival in premature babies.
RECOMMENDED READING
Cutler, J.E. (1991) Putative virulence factors of Candida albicans. Annu. Rev. Microbiol.45, 187–218.
Denning, D.W. (1991) Epidemiology and pathogenesis of systemic fungal infections in the
immunocompromised host. J. Antimicrob. Chemother.28, Suppl. B, 1–16.
Fridkin, S.K. and Jarvis, W.R. (1996) Epidemiology of nosocomial fungal infections. Clin.
Microbiol. Rev.9, 499–511.
Hogan, L.H., Klein, B.S. and Levitz, S.M. (1996) Virulence factors of medically important fungi.
Clin. Microbiol. Rev.9, 469–88.
Kobayashi, G.S. and Medoff, G. (1998) Introduction to the fungi and mycoses, in Schlaecter, M.,
Engelberg, N.C., Eisenstein, B.I. and Medoff, G. (eds) Mechanisms of Microbial Disease, 3rd
edition, Lippincott, Williams & Wilkins, Baltimore, USA.
Richardson, M.D. (1992) Fungal infections, in McGee, J.O.D., Isaacson, P.G. and Wright, N.A. (eds)
Oxford Textbook of Pathology, Oxford University Press, Oxford, UK.
Weitzman, I. and Summerbell, R.C. (1995) The dermatophytes. Clin. Microbiol. Rev.8, 240–59.
Cited By Kamal Singh Khadka
Msc Microbiology, TU.
Assistant Professor In PU, PBPC,PNC, LA, NA.
Pokhara, Nepal.
SOME SUGGESTED REFERENCES:
www.britannica.com/EBchecked/.../fungus/.../Parasitism-in-plants-and-in..
www.wisegeek.org/what-are-parasitic-fungi.htm
www.teara.govt.nz/en/fungi/page-5
website.nbm-mnb.ca › Home › Where fungi grow
www.hsu.edu/pictures.aspx?id=12367
en.wikipedia.org/wiki/Mycosis
www.ncbi.nlm.nih.gov › NCBI › Literature › Bookshelf
pathmicro.med.sc.edu/mycology/opportunistic.htm
https://www.inkling.com/read/.../classification-of-human-mycoses








The impact of fungi on humans is potentially considerable when one considers the possible targets. As
parasites fungi primarily infect plants, and the Irish famine of the 1850s in which the potato crop was
ruined by Phytopthera infestans represents an alarming example of the damaging effects fungal infection
has on foodstuffs. Two million people died during the five-year period in which the crops were lost.
Less dramatically, fungi also cause spoilage of pharmaceutical and cosmetic products, as well as
attacking the timbers of our homes.
Only a small proportion of fungi (<0.1 per cent) exist as parasites of humans and animals, fungi mostly
acting as saprophytes (organisms that absorb their organic nutrients from dead substrates). By definition,
then, saprophytic organisms are not parasitic because their nutritional sources are not alive; instead the
organisms are acting as decomposers and recyclers. As most fungal infections are acquired from an
environmental source, fungi are not obligate human parasites but, instead, human mycoses can be
considered accidental infections that are not designed to facilitate the spread of the organism to new
hosts. Hence, human to human spread is very rare for most fungal infections with the exception of the
dermatophytes.
Clinically, human fungal infections can be grouped into:
(i) systemic disease(infections of internal organs of the body), and
(ii) localised or superficial infections (infections confined to the skin or mucous membranes that do not invade into deeper tissues or organs. This classification is anthropomorphic
in that it considers the diseases as they affect man. In order to see what are the important features
of the fungi themselves, it is appropriate to group the organisms into diseases by primary
pathogenic fungi and secondary pathogenic fungi. The tiny fraction of fungi that can cause
human disease, despite the daily exposure to large numbers of airborne fungal spores, can be
taken to mean that most fungi cannot overcome human defence mechanisms.
PRIMARY PATHOGENIC FUNGI:
The fungi that are primary pathogens are those that can infect and cause disease in healthy people;
‘healthy’ in that there are no recognisable predisposing features which facilitate infection. The diseases that are seen may be systemic infections or superficial infections. This immediately demonstrates how the severity of the infection is not necessarily an indication of the pathogenic potential of the organism.
Mycosis Aetiological agent(s)
Systemic mycoses
Histoplasmosis Histoplasma capsulatum
Systemic candidosis Candida albicans
Cryptococcosis Cryptococcus neoformans
Aspergillosis Aspergillus spp.
Localised infections
Dermatophytoses Epidermophyton spp., Trichosporum spp., Microsporum spp.
Candidiasis Candida albicans
Pityriasis versicolor Pityrosporum spp
SYSTEMIC INFECTIONS:
Fungi that are able to cause systemic illness in healthy people are rare and confined to specific
geographic locations across the world. The fungus Histoplasma capsulatum causes histoplasmosis
which is endemic to certain areas in the southern states of America. Another infection is
coccidiomycosis, caused by Coccidioides immitis. Like histoplasmosis, the fungus is found between the
southern states of America, Mexico and the northern-most countries of South America. These two
infections are caused by inhalation of the fungus, which exhibits dimorphism, i.e. can exist as a yeast or
a mould. The organisms are acquired by inhalation of the conidia from soil, and develop in the lungs as
yeasts. The ability to switch between forms is seen following the change in temperature so that
Histoplasma capsulatum is a mould when grown at 25°C but grows as yeast at body temperature. This
property is then more accurately described as thermal dimorphism. The switch from being a mould in
the soil where it adopts a saprophytic existence to a yeast when at 37°C presumably favours the parasitic
existence in a warm-blooded animal. Dimorphism is a particular feature of the endemic fungi that cause
systemic infections but it is not restricted to pathogenic fungi.
SUPERFICIAL INFECTIONS: THE DERMATOPHYTOSES:
The infections caused by the group of fungi collectively termed the dermatophytesare best known by
the infection ringworm. Nothing to do with worms, ringworm is a fungal infection of the skin which
shows up as a circular area of redness in which the fungal mycelia are radially extending outwards
through the superficial skin squames. The sites of infection are reflected in the medical terms tinea
barbae (beard), tinea capitis (head), tinea corporis (body), tinea cruris (groin), tinea pedis (foot) and tinea
unguinum (nail). The different sites of infection on the body reflect the ability of dermatophytes to
invade keratinised tissues (skin, hair and nails) but no further, since these fungi have the ability to obtain
nitrogen from the keratin present only in the (dead) tissues in the body.
The dermatophytes are a group of approximately 40 species that are classified by their anamorphic
(asexual) stages. They fall into three genera: Trichophyton, Microsporum and Epidermophyton within
the Fungi Imperfecta (Deuteromycota). The ability to reproduce sexually is very rarely found in these
organisms, and this is thought to represent the intermediate transfer from environmental organisms to a
strictly parasitic existence on humans and animals. The organisms can be described according to their
ecological location:
• anthropophilic dermatophytes: exclusively infect humans,
• zoophilic dermatophytes: animal parasites that accidentally infect humans,
• geophilic dermatophytes: soil inhabitants that can infect humans and animals.
As zoophilic dermatophyte infections are transmissible from animals to humans, anthropophilic
infections are transmissible from person to person, a property unusual in human mycoses. In addition, the organisms vary in their geographical distribution with some widespread (globally) and others restricted to specific areas of the world.
As the dermatophytes infect only keratinised tissues, they do not invade living tissues. In keeping with
the descriptions of radial growth, the lesions radiate as a ring with the advancing hyphae
migrating into new tissues, and the pathology shows varying degrees of cell-mediated inflammation with
an increased rate of division and keratinisation of the skin layers. This increased cell turnover will
provide an increased supply of nutrients for the fungus. The infections with the most degree of
inflammation are the zoophilic and geophilic species, unlike the anthopophilic infections, which are
often asymptomatic. Such findings support the idea that the most host-adapted species (the
anthropophilic species) are better suited to maintaining itself within a human population.
SECONDARY FUNGAL PATHOGENS:
The three fungi that we will consider are all able to cause systemic infections, but it appears that
predisposing factors in the host are required for secondary pathogenic fungi.
It is because of the advances in medicine that opportunistic infections have become a greater problem,
both in incidence and clinical management of the patient. The increase in the number of successful
organ transplants, for example, means that such patients are at risk of developing infections due to
opportunist organisms, of which fungi have been particularly problematic. We will consider three fungi
that have become regular culprits in causing infections in patients with underlying disease: Cryptococcus
neoformans, Aspergillus spp.and Candida albicans. In all three organisms, the increased opportunities
for invading the patient have arisen from the following factors:
• increased numbers of patients with immunosuppression: naturally occurring such as AIDS or
through more successful medical immune manipulation during transplantation.
• continued use of broad spectrum antibiotics.
• increased use of intravenous lines.
• increased rates of survival in premature babies.
RECOMMENDED READING
Cutler, J.E. (1991) Putative virulence factors of Candida albicans. Annu. Rev. Microbiol.45, 187–218.
Denning, D.W. (1991) Epidemiology and pathogenesis of systemic fungal infections in the
immunocompromised host. J. Antimicrob. Chemother.28, Suppl. B, 1–16.
Fridkin, S.K. and Jarvis, W.R. (1996) Epidemiology of nosocomial fungal infections. Clin.
Microbiol. Rev.9, 499–511.
Hogan, L.H., Klein, B.S. and Levitz, S.M. (1996) Virulence factors of medically important fungi.
Clin. Microbiol. Rev.9, 469–88.
Kobayashi, G.S. and Medoff, G. (1998) Introduction to the fungi and mycoses, in Schlaecter, M.,
Engelberg, N.C., Eisenstein, B.I. and Medoff, G. (eds) Mechanisms of Microbial Disease, 3rd
edition, Lippincott, Williams & Wilkins, Baltimore, USA.
Richardson, M.D. (1992) Fungal infections, in McGee, J.O.D., Isaacson, P.G. and Wright, N.A. (eds)
Oxford Textbook of Pathology, Oxford University Press, Oxford, UK.
Weitzman, I. and Summerbell, R.C. (1995) The dermatophytes. Clin. Microbiol. Rev.8, 240–59.
Cited By Kamal Singh Khadka
Msc Microbiology, TU.
Assistant Professor In PU, PBPC,PNC, LA, NA.
Pokhara, Nepal.
SOME SUGGESTED REFERENCES:
www.britannica.com/EBchecked/.../fungus/.../Parasitism-in-plants-and-in..
www.wisegeek.org/what-are-parasitic-fungi.htm
www.teara.govt.nz/en/fungi/page-5
website.nbm-mnb.ca › Home › Where fungi grow
www.hsu.edu/pictures.aspx?id=12367
en.wikipedia.org/wiki/Mycosis
www.ncbi.nlm.nih.gov › NCBI › Literature › Bookshelf
pathmicro.med.sc.edu/mycology/opportunistic.htm
https://www.inkling.com/read/.../classification-of-human-mycoses

Comments