MICROBIAL INFECTIONS OF HUMANS(HUMAN MICROBIOLOGY CONTD..)
The normal flora offers some protection against invading pathogens. The pattern resembles the problems
of getting seeds to root in an established field of grain. The space is limited, the water and soil nutrients
are all being taken by established root systems. This protection, when applied to the intestine, is called
colonisation resistance, although the principle applies to any situation on the human body where the
normal flora limits the ability of an invading organism to gain a foothold. The efficacy of this protection
is highlighted by the disease pseudomembranous colitis(PMC). Patients with PMC develop severe
diarrhoea and have a characteristic membrane over the surface of the colon visualised by
sigmoidoscopy. PMC is caused by the multiplication and colonisation in the colon by the anaerobic
Gram positive rod Clostridium difficile. When the normal intestinal flora is disrupted by treatment with
poorly absorbed antibiotics, patients can become readily colonised by Clostridium difficile from sites
vacated by the depleted normal flora. Clostridium difficile can produce at least two protein toxins that
contribute to the diarrhoea that develops. The organism can be isolated from healthy people at low
frequency, implying that the organism either exists in very low numbers in the gut and only multiplies
when given the opportunity following antibiotic treatment, or is ingested at the appropriate time (in
hospital, for example).
Colonisation resistance applies to all sites where the normal flora is present. Within the vaginal tract,
glycogen is present in relatively high concentrations due to the resident lactobacilli that produce lactic
acid as the principle by-product of fermentation of glycogen. This production of acid lowers the pH to
acid levels as low as pH 5, an environment that is antagonistic to many bacteria.
Harbouring a normal flora is not without risks. Under normal circumstances the normal flora will most
likely not present a problem. As soon as new and unusual circumstances arise, however, some microbes
will seek to exploit a new potential site for growth and colonisation. Anyone who has cut themselves
will recognise that often the cut becomes infected. Most likely it will be a Staphylococcus aureus
infection, the organism originating from the nose. Urinary tract infections by Escherichia coli will arise
from the organisms that have passed through the gastrointestinal tract. Such organisms are thus termed
‘opportunists’; they require a breakdown in the normal protective mechanism (e.g. cut in the skin). It is
also possible to culture organisms that cause serious infections from a person who is asymptomatic. We
can conclude thus far by saying that the relationship between host and the normal flora is in equilibrium
until a perturbation of normal flora or host tissue occurs. Then the balance shifts in favour of the
bacteria, rapidly multiplying in the new environment, at least in the short term.
Knowledge of the dominant types of bacteria from the different sites of the body is essential when
looking for pathogens in clinical samples. The use of appropriate selective culture media can be employed to help isolate any pathogens in a sample that may be
dominated by normal flora (e.g. looking for salmonellae in faeces). The diagnostic microbiologist needs
to learn how to recognise and distinguish the normal flora and the potential pathogen, not least because
it is not always possible to obtain a specimen from the patient without sampling the normal flora as well
as the diseased tissue. A patient with a chest infection needs to produce a sample by coughing. The
difficulty is trying not to contaminate the sputum (from the lungs) with saliva and organisms from the
normal flora of the mouth. These procedures are possible because the organism you are looking for is
known and identifiable. Dental bacteriologists have not had it so easy. It is likely that tooth and gum
decay is caused by the collective action of members of the normal mouth/gum flora. The problem arises
because of the vast excess of glucose and other refined sugars that the modern diet provides. The marked
acidity resulting from the fermentation of the sugar erodes the tooth enamel and enables a proliferation
of anaerobic (hence, foul smelling) bacteria. It has been not been possible to convincingly identify a
single culprit responsible for dental caries.
You will have noticed that the normal flora has been contained to bacteria and yeasts that live on the
external faces of the body (where the respiratory tract, genito-urinary tract, etc. are considered external
faces). Internal organs are considered sterile. It is tacitly accepted that the presence of viruses is
abnormal (i.e. an infection). The sequencing of the human genome has unearthed numerous stretches/
fragments of past virus infections. Whether viral genome in human tissues will ever be considered
normal flora is up for debate.
One important area of concern to hospital microbiologists is the problems of infections transmitted in
hospitals. The topic brings together both the transmission of microbes and the state of the health in the
host. Does illness cause a shift in the balance between the host and the microbes they encounter?
NOSOCOMIAL INFECTIONS:
Florence Nightingale said that going into hospital should at least do the patient no harm. Today, people
often acquire an infection during their stay in hospital and these are called nosocomialinfections. The
reasons are not hard to find. Patients will likely have one or more of their natural protective mechanisms
breached. This can mean inserting an intravenous line or undergoing surgery, thereby breaching the
intact skin barrier. Alternatively, if not in addition, they might have a urinary catheter inserted, thereby
compromising the normal flushing by passing urine via the urethra. The opportunities for opportunistic
microbes to establish an infection are provided. To further increase the risk, the patient will be visited by
numerous staff and they themselves get the opportunity to touch and collect bacteria from all the other
patients. Despite rigorous hand washing it is not always possible to remove all the bacteria. Nosocomial
infections are opportunistic infections, considered separately from those infections acquired in the
community. The distinction is usually made because the compromised condition of the patient leads
them to be become infected with micro-organisms that, in healthy people, present little problem/risk.
Not that hospitals are protected from ordinary infectious diseases. The infectious diseases that infect
healthy people outside of hospitals can easily be brought into hospitals via the staff.
Infections that are acquired from external sources, i.e. are not normally resident within the host, are
termed exogenousinfections. Those infections that originate from microbes present in the host normally
are called endogenous. The terms ‘exogenous’ and ‘endogenous’ infection have particular value when
investigating nosocomial infections because many infections arise from the patient’s own flora. If the infecting agent can
be shown to be an exogenous infection it points to a problem of cross-infection. The term iatrogenic
infection applies to those infections that arise as a direct consequence of a medical or surgical procedure
(e.g. infection of a new hip joint, infections following insertion of a urinary catheter or intravenous line).
Iatrogenic infections, for example an infected intravenous line, can be either endogenous or exogenous
in origin. The implications for control are obvious, the cost is another factor altogether.
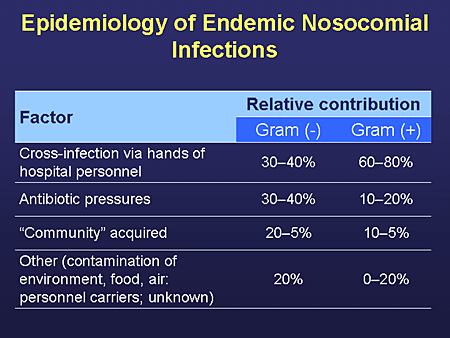
The sources of nosocomial infections are other people (staff or patients) or the patient’s environment.
This will include such diverse sources as organisms growing in ventilator tubes, or inadequately
disinfected endoscopes, through to organisms in the dust, air or food. In addition to the compromised
defences of the patient, the bacteria that cause nosocomial infections are increasingly resistant to the
action of antibiotics. Often, the organism is able to tolerate a range of different antibiotics (multiple
antibiotic resistance), posing greater problems in the treatment of the infection.
It is interesting that bacteria are the most common causes of nosocomial infections. However, more
recent trends show an increasing incidence in fungal infections. It is suggested that the advances in
medicine are paralleled by an increase in the number of infections by organisms of low virulence. The
people who previously would have died, who now are being kept alive, are liable to acquire infections
with organisms correspondingly ‘weak’. Whilst viral and fungal infections do occur, bacteria appear to
be the dominant problem. Why?
The reasons may be the source of nosocomial infections: humans and contaminated objects. Humans
carry vast numbers of microbes as normal flora, and bacteria are able to quickly grow to large numbers
in a wide variety of sites. Providing moisture and nutrients are available, bacterial growth will occur.
Being microscopic, they will not necessarily be dealt with. Fungi may be able to grow on a wider range
of substrates with less moisture (aw) but they form visible colonies of mycelia.The most frequent types of infection in hospitals occur in the urinary tract, bloodstream, the chest and in
surgical wounds. The risk of developing a nosocomial infection is related, mostly, to the severity of the
underlying disease. Patients who have impaired defences, whether they are inherited diseases of
impaired immunity or secondary to other diseases or the treatment are all called ‘immunocompromised
hosts’. The efficiency of treating the infection corresponds to the resolution of the original pathology. In
addition to the primary disease predisposing a patient to nosocomial infections, the treatment itself can
often have an effect. Drug treatment to immunosuppress patients following transplantation or treatment
of cancer with cytotoxic drugs will impair the host immune response. Antibiotic treatment itself will
disturb the normal flora (and therefore the colonisation resistance) and can select for bacteria that are
resistant to that antibiotic.
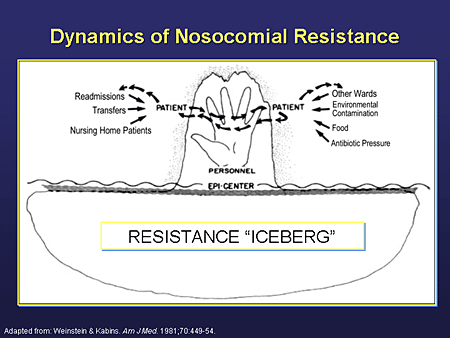
The interactions between populations defined at the start of the chapter tends to imply that they are
stable in nature. More correctly, these states will continually be challenged by new circumstances which
result in changes in the interactions. The dynamic nature of population interactions is highlighted by nosocomial infections where the condition of the host, the patient, is temporarily (we hope) altered. The
medical and surgical improvements have created a greater variety of situations for microbial exploitation with tremendous financial costs. The challenge for medicine is to attempt to treat
disease with as minimal disruption to the patient’s physiology and normal host flora as possible.
From such pragmatic issues we conclude this chapter by revisiting the biology of the micro-organism
and the reasons for parasitic infections in humans. What are the costs and benefits in choosing to infect
humans?
Cited By Kamal Singh Khadka
Msc Microbiology, TU.
Assistant Professor In PBPC, PU, PNC, LA, NA.
Pokhara, Nepal.
SOME SUGGESTED REFERENCES:
en.wikipedia.org/wiki/Hospital-acquired_infection
ceaccp.oxfordjournals.org/content/5/1/14.full
www.healthline.com/.../hospital-acquired-nosocomial-infections
emedicine.medscape.com/article/967022-overview
www.cdc.gov/hai/
www.who.int/csr/resources/publications/.../en/whocdscsreph200212.pdf
www.medterms.com/script/main/art.asp?articlekey=4590
www.mansfield.ohio-state.edu/~sabedon/biol2053.htm
www.advin.org/en/.../major-nosocomial-infections-and-their-causes.html
www.ehagroup.com/epidemiology/nosocomial-infections/
www.rightdiagnosis.com › Diseases › Nosocomial infections





Comments